
🩺 The Pulse: AI Diabetes Coaches, Faster Stroke Transfers
Plus: Adding patient context to improve output and continuity of care

1. Triage – Your Fortnightly Rundown
Hi Pulse Readers - this week, we’re diving into:
how air medical helicopter teams uses AI to speed up patient transfers,
what we know about AI diabetes coaching programme from an RCT,
and how you can add patient context in a scribe session to improve the output.
2. Case Study – Your Fortnightly Practical
Video Source: Hendrix Health
Add Context to Support Continuity of Care
Case Presentation: Dr Harry has come a long way. He has built a dedicated ADHD assessment template, used Ask Heidi to generate ad-hoc referral letters and support documents, reviewed trusted sources and guidelines before complex consultations, and managed multilingual consults with patients and their whānau, all within Heidi.
Today, he is seeing a patient for a f/u appointment. The previous visit generated a detailed note covering initial presenting complaint, history, developmental background, and a management plan. At the end of f/u consultation, Dr Harry found himself manually entering details from the prior visit to complete today's note.
He wonders whether there is a way to bring that past clinical context into the current session so that Heidi’s output reflects the full clinical picture, not just what was discussed today.
Approach: Use Heidi's context window to load relevant information from previous visits, so that the generated note is more targeted and clinically complete from the outset.
1. Open the context tab before starting the session
At the top of a new Heidi session, the default tab is the note tab. To the very left of that is the context tab. Open this before transcribing the consultation.
2. Load the relevant history into Heidi and label it clearly
Copy and paste the relevant past notes from your PMS or EHR into Heidi’s context window. Add a clear label directly above the pasted text so that Heidi understands this information is from a previous encounter and not the current one.
For example: "History from last visit: [paste prior notes here]".
Another option is uploading individual files directly from your computer by clicking the paper clip icon at the bottom left corner.
Note: You can also include other relevant background information, such as letters returned from a specialist and radiology or pathology reports. This could also be ambulance notes in an ED context.
3. Transcribe the consultation as usual
Gain consent and transcribe the visit normally. The note that Heidi generates will take into account everything in the context window alongside what was captured in the transcript. The result is a note that reflects continuity of care rather than treating the visit as a single, isolated session. You will still need to review the final note for accuracy before copying it into your PMS or EHR.
4. Keep consent in mind before loading any context
For patients known to you who have previously consented, load the prior context before the session as outlined above. However, if a patient known to you withdraws consent at the start of a f/u appointment, delete the session entirely. This will also remove any context already uploaded, respecting their decision.
For new patients, gain consent before using Heidi at all. If consent is confirmed, you can add the background clinical information into the context window after the consultation instead.
Important: Do not use the context window if the patient declines the use of an AI scribe.
Outcomes: By using the context window, Dr Harry no longer needs to manually enter a patient's history or cross-reference multiple documents. His notes already reflect the patient's relevant history, are more consistent across visits, and require fewer edits before being copied into his PMS.
For patients like his ADHD follow-ups, where continuity across multiple long appointments matters, this makes a meaningful difference to both documentation quality and admin time after the consultation.
Disclaimer: Hendrix Health is the official New Zealand partner for Heidi Health.
3. The Pulse - Your Fortnightly Update
AI Stroke Detection and Care Coordination Now Live Across 2,000 US Hospitals
Viz.ai, an AI-enabled stroke detection and coordination tool, is now in use across 2,000 hospitals in the United States. The system analyses CT scans within seconds, and when a suspected large vessel occlusion is identified, sends an alert to the treating specialist’s smartphone. This removes the manual chain of phone calls, image sharing, and delayed handovers that traditionally adds critical minutes between a scan being taken and a decision being made.
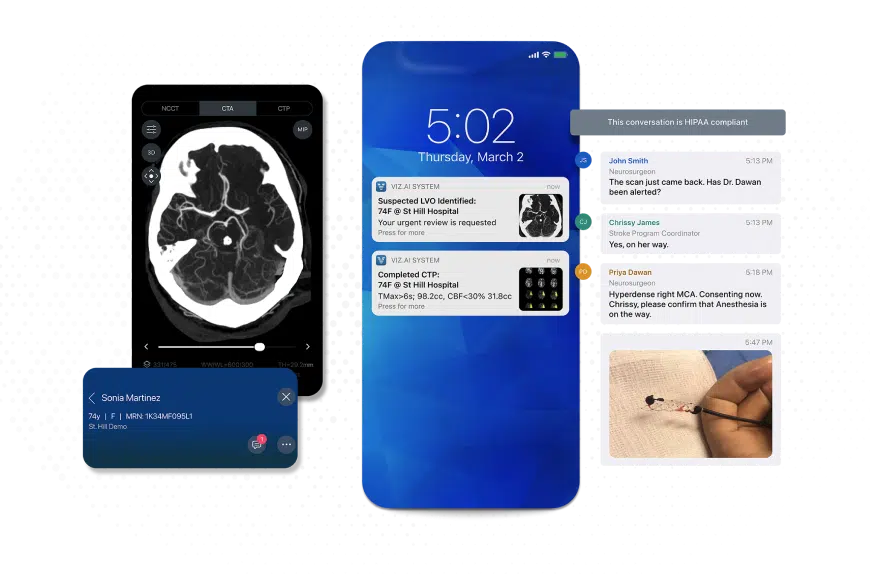
Image Source: Viz.ai
At regional hospitals that transfer stroke patients to larger centres for treatment, the system automates care-team activation and streamlines transfer coordination. The treating specialist can view the imaging and begin coordinating care within minutes of the scan being completed.
The platform has also been extended into air-medical transport. A Life Flight module, deployed as a pilot at the University of California, San Diego, allows helicopter dispatch and flight crews to join the same secure communication thread as stroke and surgical teams. This gives flight crews access to patient details, medications, and imaging findings before landing at the referring hospital, reducing the need for repeated handovers on arrival.
Key Features:
Faster transfers: At Adventist Health & Rideout, a regional stroke centre in California, the time from patient arrival to transfer out was reduced by 44%, bringing performance in line with American Heart Association benchmarks
Earlier detection: Time from scan completion to identification of a vessel occlusion fell by 84%, with specialist notification dropping from 45 minutes to 7 minutes
Low adoption burden: Life Flight teams were trained on the new module through a single 15 to 20 minute session covering workflow steps, device settings, and test activations, with no additional training required for the existing stroke team.
Clinician satisfaction: Overall satisfaction with the communication process improved by approximately 60% across all roles, with 100% of respondents preferring the new workflow
Implications for the Health System and Clinicians: For health systems that transfer stroke patients between regional hospitals and specialist centres, this is a practical example of AI reducing delays by improving how teams communicate, rather than by making clinical decisions. The value is in removing bottlenecks that slow treatment when minutes matter most.
The caution is that the strongest results come from early, single-site evaluations. Whether these gains hold consistently across different hospital networks and patient populations will need longer-term evaluation at scale.
AI-Powered Diabetes Prevention: What We Learned
On 3 April 2026, a Johns Hopkins-led phase III randomised controlled trial was presented at the NIH Pragmatic Trials Collaboratory's Grand Rounds. Published in JAMA in late 2025, the trial evaluated whether referral to a fully automated, AI-powered Diabetes Prevention Program (DPP) was non-inferior to referral to a human coach-led DPP among 368 adults with pre-diabetes and overweight or obesity across two US clinical sites, followed for 12 months.
The AI-led DPP used a reinforcement learning algorithm delivered via a mobile app and Bluetooth-enabled scale. The human-led DPP comprised four CDC-recognised programmes with the highest designation for effectiveness, delivered remotely.
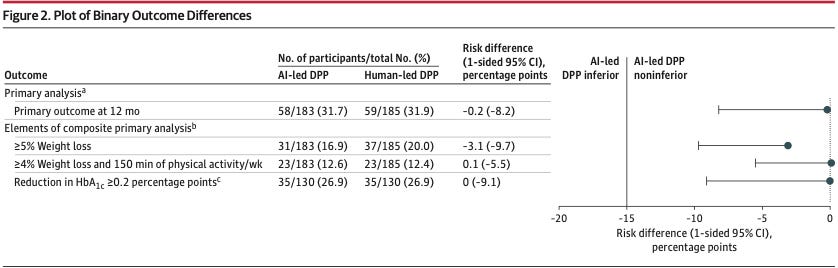
Image Source: Journal of the American Medical Association (JAMA)
Key Findings:
Non-inferiority confirmed: 31.7% in the AI-led group and 31.9% in the human-led group achieved the primary composite outcome, which included weight loss, physical activity, and HbA1c targets at 12 months. A risk difference of -0.2%, well within the pre-specified non-inferiority margin of -15%.
Higher initiation and completion with AI: 93.4% of those referred to the AI-led DPP actually began the programme compared with 82.7% in the human-led group, and 63.9% completed it compared with 50.3%.
Different engagement patterns: Among those who achieved the outcome, 74% were programme completers in the AI group compared with 56% in the human-led group, suggesting the AI programme depends more on sustained app engagement to deliver results.
No study-related adverse events, with 85.1% of participants retained at 12 months.
Implications for Healthcare Systems:
AI-based programmes can run on demand and are not constrained by the scheduling, staffing, and capacity limitations that restrict traditional DPPs. The important caveats are that participants were motivated volunteers with high educational attainment from only two sites, and the trial measured surrogate outcomes rather than diabetes incidence. The value of the AI-led DPP appears to be accessibility and reach rather than superiority over human coaching.
Read the full trial in JAMA here.
Watch the Grand Rounds session on AI for Diabetes Prevention here.
4. Vitals – Quick Bytes
Western Australia Funds AI Pilot to Improve Hospital Workflow and Efficiency
The Western Australian Government is investing A$700,000 in an AI pilot at Royal Perth Hospital to predict length of stay and streamline hospital workflows ahead of the 2026 winter season. The system will schedule tasks including medical imaging, laboratory tests, pharmacy medication packs, and discharge summaries, with the aim of improving bed availability and reducing delays. A new system-wide data platform will feed live dashboards for the State Health Operations Centre to track demand, capacity, and patient movement across the public health system. If successful, the pilot may be scaled across multiple hospitals and integrated with other digital health initiatives.
US Survey Finds Public Openness to AI in Healthcare is Declining
A national survey of 1,007 US adults commissioned by The Ohio State University Wexner Medical Center found that only 42% are open to AI being used in their healthcare, down from 52% in 2024. The belief that AI can improve healthcare efficiency also fell, from 64% to 55%. At the same time, 51% of respondents reported using AI to make a health decision without consulting a medical professional, and 62% use AI to understand symptoms before deciding whether to seek care. Researchers noted the decline is consistent with the natural technology hype cycle and expect trust to stabilise as the true use cases for AI in healthcare become clearer. (medicalxpress.com)
We’d love to hear your thoughts, so join the conversation by leaving a comment below:

Stay tuned for more insights in the next edition of The Pulse.
Have a great day & see you in two weeks!
Your Hendrix Health Team