
🩺 The Pulse: America's Virtual Hospital System and AI in Cardiovascular Care
Plus: Using Heidi to manage multilingual consultations

1. Triage – Your Fortnightly Rundown
Hi Pulse Readers - this week, we’re diving into:
expansion of AI-assisted hospital room technology across the US,
what a large RCT tells us about AI in stroke care decision support,
and how you can make the most out of Heidi’s functions when you’re speaking multiple languages during a consultation.
2. Case Study – Your Fortnightly Practical
Video Source: Hendrix Health
Managing Multilingual Consults with Heidi
Case Presentation: Last time, Dr Harry used Heidi Evidence to review trusted sources and guide his approach to a clinical question. It is quick, reliable, and completely ad-free to get the answers he needs.
Today, he is seeing a patient whose mother speaks only Cantonese, while the daughter speaks English. While being fluent in both English and Cantonese, Dr Harry wants to communicate clearly with both patient and whānau, but without doubling his workload by manually translating explanations or writing separate documents.
He considers whether Heidi can support multilingual transcription and communication within the same session.
Approach: Changing Heidi’s input language settings to capture multilingual consults and using Ask Heidi’s translation capability generate patient-friendly explanations in multiple languages.
1. Set input languages before starting the consult
Adjust Heidi’s input settings to match the languages spoken in the room, for example English and Cantonese. This allows Heidi to process mixed-language conversations without breaking workflow or requiring separate documentation. Heidi can listen for up to 3 languages when transcribing. For example, English, Te Reo Māori, and Cantonese.
2. Conduct the consultation naturally
Allow the conversation to flow between you, the patient, and family members in their preferred languages. There is no need to force everything into English, as it reduces accuracy and rapport.
Heidi captures the consult and generates a structured note in English (or any output language you select) for clinical documentation.
3. Generate a patient-friendly explanation
After completing the consult, click the Ask Heidi bar at the bottom of your screen:
“Create a simple patient explanation of the diagnosis and management plan in English.”
This ensures clarity, especially for complex conditions like ADHD or mental health presentations.
4. Translate for the patient and whānau
Follow-up in Ask Heidi with: ”Translate this explanation into [language of your choice].”
Then, review the output before providing both versions of the patient explainer to the patient and their family.
Important: Do not rely on this workflow if you cannot verify the translation yourself. You remain responsible for accuracy and clinical safety in any case.
Outcomes: Dr Harry is now able to manage multilingual consults without slowing down or compromising communication quality. Instead of fragmented conversations and duplicated admin, he delivers clear, structured explanations in both languages within minutes. This improves patient understanding, supports whānau involvement, and reduces the risk of miscommunication.
Dr Harry maintains a single, efficient workflow while adapting to the diverse patient populations in Aotearoa New Zealand.
Disclaimer: Hendrix Health is the official New Zealand partner for Heidi Health.
3. The Pulse - Your Fortnightly Update
AI-Assisted Hospital Rooms Expand Across 25 Hospitals (WVU Health System)
WVU Health System has begun rolling out AI-assisted “intelligent hospital room” technology across all 25 hospitals in its network, covering more than 3,000 beds across West Virginia, Ohio, Pennsylvania, and Maryland. The rollout is delivered through a partnership with hellocare.ai, and is one of four new partnerships the AI company has announced with US health systems in 2026.

Image Source: Hellocare.ai
When a patient is admitted, bedside devices, video systems, and monitoring tools connect into a single virtual care platform that is integrated with the Epic EHR. The platform combines AI, secure video collaboration, real-time communication tools, and clinical workflow integration to support patient observation, fall prevention, remote consults, and communication between care teams, patients, and families.
Virtual care teams, including remote nurses, can then support bedside staff through virtual nursing workflows, while clinicians and specialists can also join care remotely through virtual rounding and telehealth.
Key Features:
Virtual nursing support: Remote nurses support bedside teams through virtual nursing workflows and communication.
AI-assisted patient monitoring: Continuous observation may help detect deterioration earlier and supports fall prevention.
Integrated communication: Video, messaging, and EHR integration allow easier communication between care teams, patients, and families.
Virtual rounding and telehealth: Specialists can review and contribute to care without being physically on-site.
Large-scale rollout: Deployment across 25 hospitals and 3,000+ beds signals standardised infrastructure rather than pilot-stage experimentation
In some hospitals, additional features such as digital whiteboards, door signage, and patient infotainment systems are also being added.
Implications for the Health System and Clinicians:
This reflects a broader shift in how inpatient care is organised, separating physical presence from clinical contribution. Tasks that do not require hands-on care, such as monitoring, communication, and routine support activities, can now be delivered remotely.
For clinicians, the potential value is better communication, more support with monitoring, and less pressure on bedside teams. For health systems, the appeal is clear: improving patient safety and workflow efficiency without relying only on traditional staffing models that are vulnerable to shortages.
The rollout is large and the platform is clearly integrated into hospital workflows, but there is no published data on staff and patient outcomes. The real question is whether these benefits hold up in practice.
AI Stroke Decision Support: What a 21,000-Patient Cluster RCT Reveals
A large cluster-randomised clinical trial in The BMJ evaluated an AI-based clinical decision support system (CDSS) for acute ischaemic stroke across 77 hospitals in China, involving 21,603 patients admitted within seven days of symptom onset.
The system combined AI-assisted imaging analysis, classification of stroke cause, reminders for pending assessments, and evidence-based treatment recommendations during admission and at discharge.
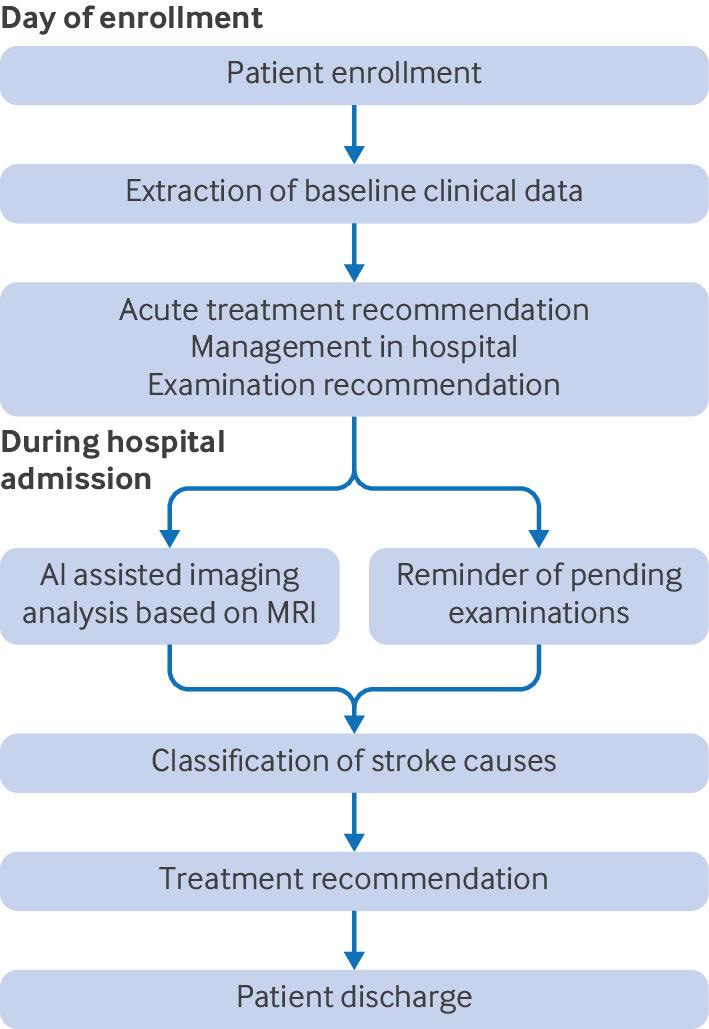
Image Source: the BMJ
Key Findings:
Fewer new vascular events at three months: The primary outcome, a composite of ischaemic stroke, haemorrhagic stroke, myocardial infarction, or vascular death, occurred in 2.9% of patients in CDSS hospitals versus 3.9% in usual care hospitals, a relative risk reduction of about 26%.
Improved stroke care quality: The composite adherence score for evidence-based stroke care was higher in the intervention group, 91.4% versus 89.8%. The biggest gains were seen in secondary prevention and inpatient care measures, including dual antiplatelet therapy, anticoagulation for atrial fibrillation, dysphagia screening, and DVT prophylaxis, where baseline adherence was lower.
Benefits persisted over 12 months: New vascular events remained significantly lower at six months, 3.4% versus 4.8%, and at 12 months, 4.0% versus 5.5%, driven primarily by reductions in recurrent ischaemic stroke.
No clear difference in disability, mortality, or bleeding: Despite fewer recurrent vascular events, the trial did not find significant differences in disability, all-cause mortality, or moderate to severe bleeding, which suggests the system improved secondary prevention without increased safety risk.
Implications for Healthcare Systems:
AI-based decision support can improve stroke care quality and reduce recurrent vascular events when embedded directly into routine workflows, particularly in time-critical, protocol-driven pathways like stroke. A CDSS can help clinicians follow guidelines more consistently and reduce variation in care at scale. The caution is important: this study was conducted at the hospital level rather than individual patients, in a population where most strokes were relatively mild, and it did not assess cost-effectiveness or include thrombectomy decision-making. As such, further validation across different health systems and patient populations will be needed before widespread adoption.
Read the full study here.
4. Vitals – Quick Bytes
New Zealand’s National Diabetes Roadmap Signals AI-Enabled Screening
Health New Zealand has launched a National Diabetes Roadmap that includes exploring AI in diabetic retinopathy screening and piloting retinal photo screening in primary care settings. The strategy also aligns HbA1c thresholds with international standards to support earlier detection and intervention. Alongside workforce expansion and community-based care, this signals a shift toward more technology-enabled diabetes management at a national level. However, this remains policy direction rather than proven deployment. The takeaway is simple: AI is now part of the national plan, but impact will depend on whether these pilots translate into real-world reductions in complications.
Studies on AI-Enabled Stethoscopes Suggest Better Detection, But Implementation Limits Impact
Two recent studies examined whether AI-enabled stethoscopes can improve detection of cardiovascular disease in primary care. In a prospective study of 357 at-risk patients, AI-augmented digital auscultation substantially improved sensitivity for moderate-to-severe valvular heart disease compared with standard auscultation, detecting 12 previously undiagnosed cases versus 6 with routine care, though with lower specificity.
Meanwhile, the larger TRICORDER cluster-randomised implementation trial across 205 UK primary care practices found no significant increase in population-level detection of heart failure, atrial fibrillation, or valvular heart disease after 12 months, largely because real-world uptake was inconsistent and use declined over time. Taken together, it is clear that the technology itself performs well. But to deliver real clinical impact also relies upon workflow integration, sustained clinician use, and access to follow-up testing and specialist care.
We’d love to hear your thoughts, so join the conversation by leaving a comment below:

Stay tuned for more insights in the next edition of The Pulse.
Have a great day & see you in two weeks!
Your Hendrix Health Team