
🩺 The Pulse: Tikanga-Grounded Copilot Rollout and Autonomous AI Anaesthesia
Plus: Getting started with Heidi's new wearable microphone

1. Triage – Your Fortnightly Rundown
Hi Pulse Readers - this week, we’re diving into:
Health NZ's culturally grounded “BroPilot” rollout in Hauora Māori Services,
how an AI sedation system performed against anaesthetists in a multicentre RCT,
and how to set up your new Heidi Remote quickly.
2. Case Study – Your Fortnightly Practical

Image Source: Heidi Health
Setting Up Heidi Remote for the First Time
Case Presentation: Last time, Dr Harry used Heidi Tasks to automate his follow-up to-do list.
This week, his practice asked him to take over the Friday rest home visits, covering 8 to 10 elderly residents. So far, he has been balancing his laptop on a bedside table or propping his phone against a fruit bowl. He also noticed some of his patients glance at his phone with skepticism even after giving consent.
He has just received Heidi Remote, Heidi’s new wearable microphone, and wants to set it up before next Friday.
Approach: Pair Heidi Remote to the Heidi app, wear it during the round, and let audio sync automatically.
1. Confirm compatibility and charge
Heidi Remote pairs with the Heidi iOS, Android, and Desktop apps (not yet the web browser version). Use the supplied charging cable rather than a fast charger. A full charge takes about 1.5 hours and gives 14 hours of use.
2. Power on, pair, set a default template.
Hold the Power button for 2 seconds until the LED turns solid white. Keep the device within arm's reach of your phone, then in the Heidi app go to Settings, then Add Device, and follow the prompts. Set a default note template (for example, a rest home progress note) that all synced sessions will use.
3. Wear it and record
Clip Heidi Remote high on your chest or top pocket, facing outward. At each bedside, gain consent, then press the Record button once to start (LED red), again to pause (orange), and hold for 2 seconds to stop and save (white).
Important: Heidi advises keeping the device away from anyone with implanted pacemakers or defibrillators (magnetic components).
4. Let it sync
Out of Wi-Fi range, Heidi Remote keeps recording offline and stores audio on-device (32GB, over 100 hours of capacity). Back in range, sessions sync automatically into the Heidi app. Link each session to the resident and review the notes.
Note: Heidi Remote is in Early Access, so specifications may change. Heidi classifies it as an audio peripheral, with the clinician remaining responsible for clinical accuracy, consent, and data compliance.
Outcomes: Dr Harry's Friday visits run without a laptop or a propped-up phone. He clips Heidi Remote to his collar, presses one button at each bedside, and stays present with the resident.
By the time he reconnects at the practice, audio is syncing. He links each session, reviews, and copies into his PMS. He drives back to the practice with the documentation already done.
Disclaimer: Hendrix Health is the official New Zealand partner for Heidi Health.
3. The Pulse - Your Fortnightly Update
Hauora Māori Services Customises Microsoft Copilot into "BroPilot", Grounded in Tikanga Māori
Health New Zealand has adapted Microsoft 365 Copilot into a culturally grounded AI tool called BroPilot, built within Hauora Māori Services and shaped around tikanga Māori. The programme used Dame Naida Glavish's Tikanga Best Practice Guidance as its foundational document. More than 200 staff with knowledge of Māori tikanga contributed to developing 16 measurable standard operating procedures grounded in Māori culture and values.

Image Source: news.microsoft.com
The rollout sits under HealthX, Health NZ's programme for scaling digital and AI solutions, which began in August 2025. Since January 2026, more than 2,050 Copilot licences have been issued, with deployment sequenced to leadership and digital teams first.
Adoption is supported through twice-weekly drop-in sessions where staff bring real work. Within BroPilot, kaimahi have built their own role-specific AI personas, such as Smartmāori for research, Nanny for kaupapa advice, Coco for day-to-day tasks, and Doc for executive-level documents.
Key Features:
Cultural foundation: 16 standard operating procedures developed with input from over 200 staff with Māori tikanga knowledge.
Practical adoption model: Drop-in sessions every Monday and Wednesday let staff bring real work into a secure enterprise environment.
Personalised AI personas: Staff build their own agents within BroPilot for specific functions, from research and kaupapa advice through to admin and document drafting.
Workflow applications: Reported uses include summarising long documents, extracting actions, clarifying responsibilities, improving report structure, and turning dense material into clearer outputs.
Scale of rollout: Over 2,050 Copilot licences issued since January 2026 under HealthX, with deployment continuing across an organisation of more than 90,000 staff.
Implications for the Health System and Clinicians: For clinicians and practice managers watching AI rollouts in Aotearoa, BroPilot is a useful local case study in how adoption tends to succeed or fail on the human side, rather than the technology. The combination of cultural grounding, enterprise governance, and learning through real work shows what a thoughtful rollout can look like inside a complex public health system. We look forward to seeing outcomes data on productivity, retention, and clinical or administrative workflow.
AI-Driven Anaesthesia System for GI Endoscopy: a 418-Patient Multicentre RCT from China
A multicentre randomised controlled trial in npj Digital Medicine tested an AI system that automates sedation during gastrointestinal endoscopy. Known as AAS-GE, this automated anaesthesia system uses reinforcement learning to adjust the sedative drug, ciprofol, in real time based on patient vital signs.
The trial ran across five hospitals in China between January and August 2025, enrolling 418 adults with low anaesthetic risk, aged 18 to 65 undergoing routine GI endoscopy. Half received AI-controlled sedation, the other half clinician-managed anaesthesia. The primary safety outcome was hypoxaemia, defined as oxygen saturation < 92% at any point during the procedure.
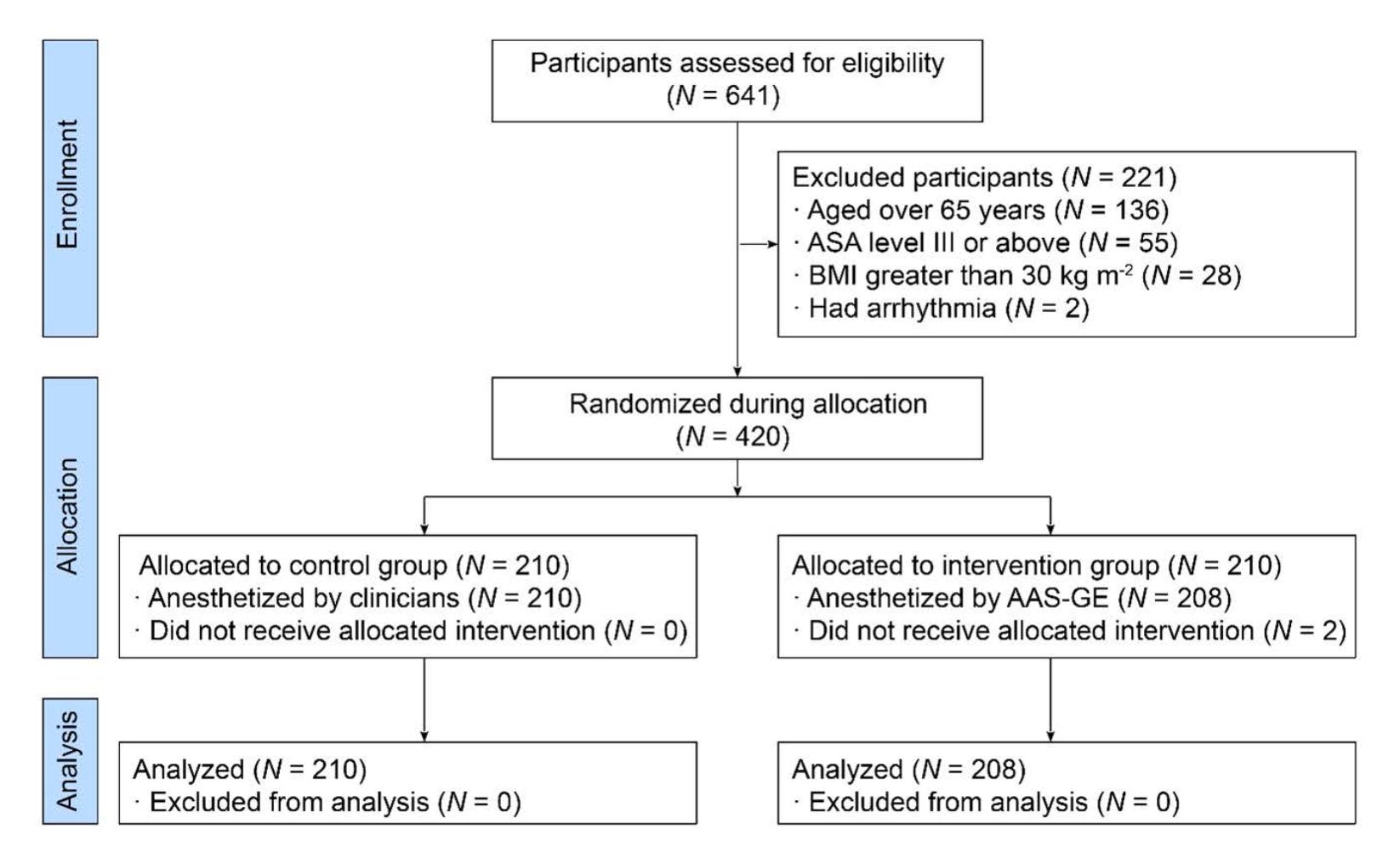
Image Source: npj Digital Medicine
Key Findings:
Non-inferior safety: Hypoxaemia rates were almost identical between groups (14.42% vs 14.29%), with no significant differences in severity or the lowest oxygen levels recorded.
Faster induction without higher drug use: The AI group reached anaesthesia depth significantly faster (1.55 vs 1.90 minutes), with no significant differences in total ciprofol doses or recovery duration.
More intraoperative body movement: Body movement was significantly more frequent in the AI group (17.79% vs 6.67%). Affected patients received lower maintenance doses, suggesting the AI kept patients in a slightly lighter state of sedation than clinicians would.
No difference in other adverse events: Rates of swallowing, jaw lifting, coughing, vasopressor use, and supplemental oxygen were similar between groups.
Implications for Healthcare Systems:
This trial moves AI a step beyond decision support and into autonomous clinical delivery. The AI matched anaesthetists on safety while being faster, which is meaningful given global anaesthetist shortages and rising procedural volumes. However, it is important to note that the model was trained on data from a single hospital, and the more frequent body movement suggests it dosed more cautiously than clinicians would. Human-in-the-loop oversight was mandatory throughout, with anaesthetists retaining full override authority.
Read the full trial here.
4. Vitals – Quick Bytes
Te Aho o Te Kahu Pilots AI-Assisted Pathology Reporting in Three NZ Labs
An AI-assisted Structured Anatomical Pathology (ASAP) application went live with Pathologists at Waitematā, Christchurch, and Dunedin laboratories as part of New Zealand's national Cancer Control Agency’s CanShare programme. ASAP uses AI to draft pathology reports and tag key clinical details with SNOMED CT, a standard coding system that makes cancer information easier to share and reuse across the health system. The pilot is testing how well ASAP fits into pathologists' day-to-day work, the quality of the reports, and how quickly coded results can be shared with treating teams. Delivered with Health NZ Te Whatu Ora, AWS, and Deloitte, the pilot runs for two months and will inform whether AI-assisted structured reporting has a wider role in Aotearoa.
Robotic Phlebotomy Achieves 94.5% First-Stick Success in Dutch Multicenter Trial
A multicenter trial evaluated an autonomous robotic phlebotomy device (Aletta, by Vitestro) across three Dutch hospitals, enrolling 1,633 patients for routine outpatient blood draws. The device uses near-infrared imaging, ultrasound, and Doppler to locate a vein, then performs the venipuncture itself. First-stick success was 94.5% overall, holding up in patients with difficult venous access (92.7%), obesity (97.4%), and those aged 65 or older (93.4%). Adverse events were mild and uncommon (0.6%), and 82% of surveyed patients said they would prefer the device or had no preference over manual phlebotomy.
Caveats: the trial was manufacturer-funded, several authors are company employees, the routine-use cohort had no manual control group, and 6% of patients were screened out because no suitable vein could be identified.
We’d love to hear your thoughts, so join the conversation by leaving a comment below:

Stay tuned for more insights in the next edition of The Pulse.
Have a great day & see you in two weeks!
Your Hendrix Health Team