
🩺 The Pulse: AI Skin Cancer Triage Across the UK, Predicting Heart Failure with AI Algorithm
Plus: Finding ready-made ACC report templates in Heidi's Community Library

1. Triage – Your Fortnightly Rundown
Hi Pulse Readers - this week, we’re diving into:
how an AI tool now triages suspected skin cancer referrals across 26 NHS trusts,
what an Australian trial reveals about predicting future heart failure from a routine echo with AI,
and how you can find ready-made ACC report templates in Heidi’s Community Template Library.
2. Case Study – Your Fortnightly Practical
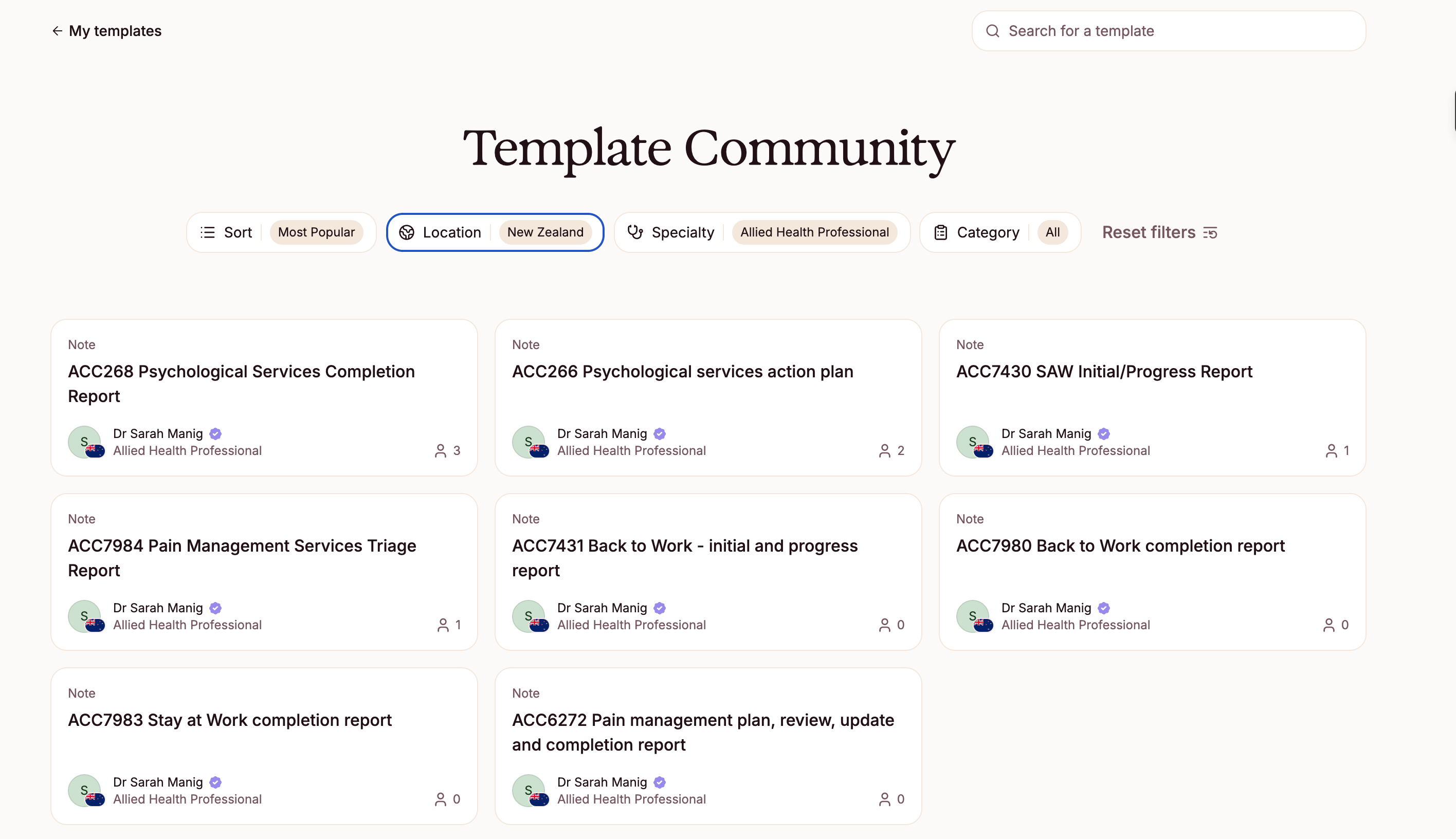
Image Source: Heidi Health
Streamlining ACC Documentation with Heidi Templates
Case Presentation: Last time, Dr Harry helped his practice manager put a shared AI policy in place: a clear register of approved tools, rules about what patient information can go where, and a named owner to keep it current.
This fortnight, he is back to his own workflow. A patient with a work-related shoulder injury needs an ACC back-to-work assessment report before returning to a labouring role. He has completed a few of these this year, but not often enough to have the structure memorised: which headings ACC expects, which functional categories apply, how detailed the narrative needs to be.
Before starting another one from scratch, Dr Harry opens Heidi's Community Template Library to check whether a suitable starting point already exists.
Approach: Search the Heidi Community Template Library for pre-built ACC templates, save the relevant ones to your personal library, and adjust them before use.
Open the Community Template Library and filter for ACC templates
Navigate to the Templates section in Heidi and select the Community Template Library. Apply both the “allied health professional” and “new zealand” filters to narrow results to ACC-relevant templates for Aotearoa. The filter returns 8 templates covering the ACC reports that carry the heaviest documentation load in allied health practice: back-to-work reports, stay at work assessments, pain management plans, and psychological services documentation.
Preview and save to your personal library
Click into each template to review its structure and format before saving. Saved templates appear alongside your existing Heidi templates. You can save more than one and label them by form type for easy access.
Note: Templates in the Community Library are available on action credits in the free version of Heidi, or unlimited on any paid plan.
Adjust the template to your documentation style
Community templates are starting points. Open the template settings to edit headings, adjust output instructions, or add practice-specific sections. If your ACC contract requires particular headings or response formats, build those in now. This avoids manual edits each time.
Use the template in your next ACC session
Select the template at the start of your ACC-related consultation. As with all Heidi-generated notes, review the output before copying it into your PMS or filing with ACC.
Important: ACC documentation carries legal and contractual weight. Review every generated note before submission. You remain responsible for the accuracy and completeness of all forms filed under your name.
Outcomes: Instead of rebuilding report structure from scratch, Dr Harry now has a template already shaped around New Zealand's ACC documentation requirements. The layout is handled. He focuses on the clinical content.
For physiotherapists, psychologists, and OTs in ACC-contracted practices, the same library holds templates covering the forms that generate the most consistent overhead week to week. The 8 templates were built by Dr Sarah Manig, with more to follow as the library expands.
Disclaimer: Hendrix Health is the official New Zealand partner for Heidi Health.
3. The Pulse - Your Fortnightly Update
AI Skin Cancer Triage Now Used Across 26 NHS Trusts
Bradford Teaching Hospitals NHS Foundation Trust joined 25 other trusts across the UK to use an AI tool named DERM (Deep Ensemble for Recognition of Malignancy), to triage suspected skin cancer referrals at St Luke's Hospital. Bradford is the first in West Yorkshire to adopt it.

Image Source: Med-Tech Insights
Patients referred by their GP enter a new teledermatology service, where staff photograph suspicious lesions with a dermatoscope attached to their phone lens, and DERM’s AI software returns a triage recommendation in seconds. Flagged lesions go to a consultant dermatologist in an adjoining one-stop clinic; benign cases are reassured and discharged.
Bradford receives around 5,000 skin cancer referrals a year but only 8% prove malignant, so DERM clears the benign majority off the two-week pathway to protect specialist time.
Key Features:
Scale of adoption: DERM is currently deployed across 26 NHS trusts, including multiple teaching hospitals.
Regulatory standing: NICE conditionally recommended DERM in May 2025 for three years while evidence is gathered, and an NHS England report found it could be used autonomously, with a negative predictive value of 99.8% versus 98.9% for dermatologist assessment.
Efficiency and cost: Estimated savings of around £86 per case and a £1.70-2.30 return for every £1 spent, mainly from fewer face-to-face reviews and biopsies.
One-stop pathway: A flagged lesion can be excised at the same visit, sparing many patients weeks of repeat biopsies.
Built-in safeguards: Risk-based logic routes each lesion to the safest pathway, and Bradford’s first-year data will be independently evaluated by the regional Cancer Alliance.
Implications for the Health System and Clinicians: Since a 2022 pilot in London, DERM has seen 260,000+ patients and found close to 20,000 cancers. For Aotearoa, where melanoma rates are among the world’s highest, triaging the benign majority off urgent lists is the model to watch, and the MedTech company has signalled expansion into Australia.
However, DERM is still in an evidence-gathering phase: the NICE recommendation is conditional, with company-reported headline figures, and less certain performance for black and brown skin requiring extra clinician review. Whether autonomous triage holds up safely across diverse populations, and whether the promised community and GP rollout arrives, will decide if it becomes standard or stays a supervised pilot at scale.
Predicting for Future Heart Failure from a Routine Echo: What an Australian AI Trial Shows
A blinded, retrospective study in JACC: Heart Failure tested whether AI could turn a routine echocardiogram into a screen for future heart failure. The Australian-led team applied an AI risk algorithm built on the National Echo Database of Australia, to baseline echoes of 453 patients discharged in pre-symptomatic heart failure (stage A or B), then tracked who progressed to symptoms.
Prevention means finding at-risk patients before symptoms take hold, yet predicting who progresses is difficult. The algorithm scores risk from the measurements in an existing echo report, so it needs no new test.
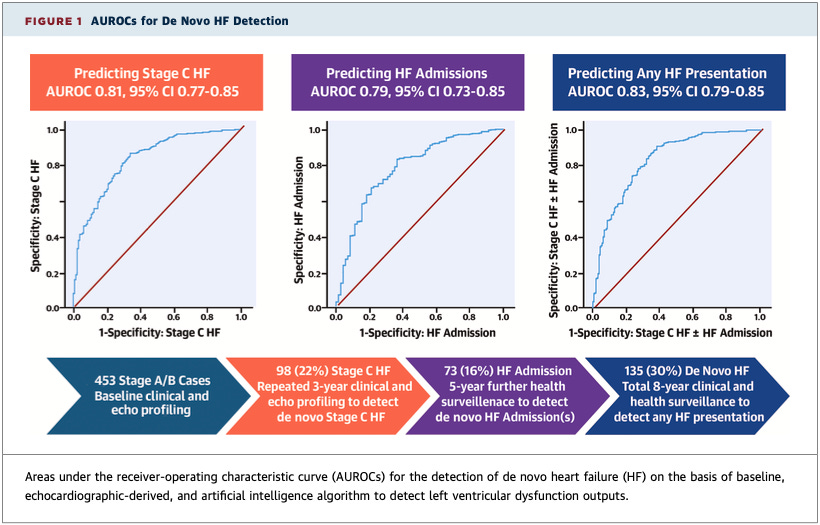
Image Source: Journal of the American College of Cardiology (JACC Journals)
Key Findings:
Accurate risk stratification: From echoes taken three or more years earlier, it predicted who would develop symptomatic (stage C) heart failure with an AUROC of 0.81 (1.0 is perfect), rated excellent.
Predicted who would be admitted: It was nearly as accurate at predicting future heart failure admissions (0.79), and most accurate (0.83) at predicting either event, new heart failure or an admission.
Beat the standard risk tool: Today’s standard calculator (PREVENT-HF) worked for only 54% of patients, needing inputs many lacked, and was less accurate (0.73); the AI scored nearly all and predicted better.
Progression was common: Though all began symptom-free, within three years 1 in 5 (21.6%) developed symptomatic heart failure, and nearly 1 in 3 (29.8%) developed it or were hospitalised, despite specialist care.
Implications for Healthcare Systems:
For prevention, the appeal is clear: a score from echoes already being performed could help cardiology and primary care flag patients for earlier guideline-directed therapy, before symptoms appear. On the other hand, this was a small, single-centre, retrospective proof-of-concept not powered for these predictions, and funded by Echo IQ, the algorithm's developer, with several authors paid as consultants. Survival bias and advances in heart failure therapy since the original trial temper the results. A risk score is only the beginning; whether acting on it prevents progression cost-effectively is still unanswered.
Read the full study here.
4. Vitals – Quick Bytes
Monash Health and Heidi Trial Real-Time AI Translation in Hospitals and Clinics
Monash Health, one of Australia's largest health services, has partnered with Heidi to co-develop and trial a clinical-grade, real-time AI translation tool across its hospitals and clinics. The tool supports communication between patients, families and clinicians, initially covering 10 commonly spoken languages, in a network where 45% of patients speak a language other than English at home. It is built to hospital standards for privacy, security and clinical safety. Professional interpreters will continue to be used for complex care or sensitive conversations, with the trial testing where AI can safely support everyday communication rather than replace existing services.
Sydney's START-AI Model Predicts Inpatient Admission in a 163,000-Case ED Study
A study in Emergency Medicine Australasia used ensemble machine learning to extend START, an admission risk tool already used in New South Wales patient flow systems, into START-AI. Drawing on 162,915 adult ED presentations from a single Sydney tertiary hospital (27% admitted), the model combined the original START score with vital signs, blood tests, CT orders and free text from triage and clinical notes to predict who would be admitted. The full model predicted admission more accurately than START alone (AUROC 0.88 versus 0.77), and reached 0.93 for predicting ICU admission or death. The authors note this single-centre study only derived and internally validated the model, which is designed to support senior ED decision-making rather than replace it. Prototype development and prospective evaluation are still needed before clinical use.
We’d love to hear your thoughts, so join the conversation by leaving a comment below:

Stay tuned for more insights in the next edition of The Pulse.
Have a great day & see you in two weeks!
Your Hendrix Health Team